Case: 58 year old male with history of "CHF" presents to ER with shortness of breath. On exam patient appear to have classic signs of 'exacerbation of CHF'. Patient also complain of nausea, vomiting, diarrhea and abdominal pain. Also, patient sees everything green, double and blurred ! Labs are not back yet but following EKG is obtained. With above history, what is your suspicion ?
Answer: Digoxin Toxicity
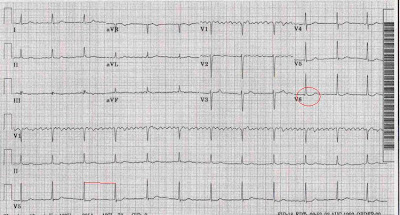
The 3 major hallmarks on EKG of Digoxin toxicity
- accelerated junctional rhythm, also called "regularized Atrial Fibrillation"
- ST segment sagging (This finding is not indicative of toxicity unless other signs present)
- a shortened QT interval
First rule is - Comparison with previous EKGs.
Many times, its hard to find any specific EKG sign. Digoxin toxicity may cause any dysrhythmia including paroxysmal atrial tachycardia with 2:1 block, accelerated junctional rhythm, or even torsade de pointes. Premature ventricular contractions (PVCs) are very common. Bigeminy or trigeminy can be seen frequently. Sinus bradycardia, other bradyarrhythmias, First- and second-degree AV block, complete AV dissociation, and third-degree heart block are very common too.
Cardiac arrest - Ventricular tachycardia,asystole, ventricular fibrillation - is hard to rescue and usually fatal.
No comments:
Post a Comment